
Change is Coming for Physician Compensation Data
Darcy Devine • May 6, 2016

Back in 2004, CMS provided the healthcare industry with two methodologies
for calculating fair market value hourly rates for physician services.
First, CMS said that you could pay a physician less than or equal to the average hourly rate being paid to emergency room physicians in the relevant market, provided there were at least three hospitals in the market.
This methodology wasn’t used that often. Not many people had access to the specific market data that was needed for the calculation. And, if you could get the data, there were concerns about meeting the conditions necessary to fall within the antitrust safety zone.
Alternatively, CMS said that you could derive a fair market value hourly rate by using six specific national physician compensation surveys. To do this, you averaged the median for the specialty (or general practice) from at least four of the surveys. Since the benchmarks were for annual compensation, you converted them to an hourly rate by dividing by 2,000 hours.
The introduction of this safe harbor increased the healthcare industry’s reliance on compensation surveys. I’m sure sales skyrocketed for the surveys CMS identified in the regulations.
In 2007, CMS eliminated the safe harbor. There were too many complaints. One of the surveys had stopped being produced; one of the surveys was not being sold to the public; and the others were too expensive.
A lot has changed over the last ten years. Using multiple, objective, independently published salary surveys to evaluate and support fair market value for physician services has not. However, I believe there is going to be a significant change in how the healthcare industry gets physician compensation data.
One of the biggest reasons for this is that the compensation data that was too expensive ten years ago is even more expensive today. In 2004, it cost about $2,000 to buy the four surveys needed for the safe harbor calculation. Today, the same collection can cost a consulting firm nearly $50,000. This is a necessary expense for those of us who specialize in physician compensation. For others, it is no longer affordable.
Online information companies like Medscape are starting to fill in the hole. Medscape has surveyed physicians for several years now about how much they earn and how much they work. Summary results are available at no charge on the company’s website. If Medscape decides to release more details about the 19,200 physicians that respond to its survey, it could become one of the most relied upon resources for physician compensation data in the healthcare industry.
The internet provides a wealth of other quality data resources, too. Certain online databases actually provide more detail than the well-known physician compensation surveys – although the data can be hard to find, and it doesn’t always come in the neatest package. But no doubt, current market dynamics will change where and how the healthcare industry gets physician compensation data.

We ranked the 30 largest healthcare services and information technology deals of 2018, according to our database, by valuation multiple. The lowest reported price to EBITDA multiples (10x or lower, sorted alphabetically) are listed below.

We ranked the 30 largest healthcare services and information technology deals of 2018, according to our database, by valuation multiple.

We ranked the 30 largest healthcare services and information technology deals of 2018, according to our database, by valuation multiple. The highest reported price to EBITDA multiples (15x or higher, sorted alphabetically) were as follows:

Healthcare services organizations rely on a variety of intangible assets to create business value, including patient and customer relationships, medical records, trade names, assembled workforce, licenses and certifications, non-compete clauses, proprietary technology, software, and others.

For those of you who’ve been involved in a transaction where the only asset transferred is a certificate of need, you’ve probably found that market data is scarce for CON-only deals.

CON Laws, Scope of Practice Restrictions, and Provider Non-Compete Clauses Targeted in New Trump Adm
On Monday, December 3, 2018, the Department of Health and Human Services (HHS) – in collaboration with the Departments of the Treasury and Labor, the Federal Trade Commission, and several offices within the White House – released a report detailing recommendations for improving choice and competition in the healthcare industry.

One of the questions we get asked a lot is how valuations have changed over time.

One of the many benefits of tracking healthcare transactions closely and maintaining a very large database of deals where we can get reliable price to EBITDA and revenue multiples is that it provides insight into profit margins for segments where other financial benchmarking information is sparse.

The most important component of a valuation of an accountable care organization (or other multi-provider network that relies on risk-based shared savings models) is the revenue forecast, which involves “probability-adjusting” future shared savings payments in some manner.
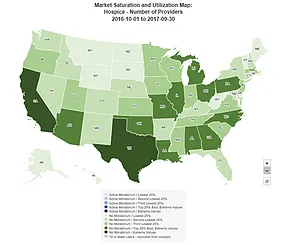
CMS' offers a helpful online tool that shows provider market saturation levels at the national-, state-, and county-levels for the following health services:

