
Commercial Reasonableness and Physician Employment Arrangements: Two Points of View
Darcy Devine • July 28, 2018
A common assignment for a health care valuation consultant is to review a proposed employment agreement between a hospital (employer) and a physician (employee) and determine whether the compensation described in the agreement is consistent with fair market value (FMV). In addition to reviewing the agreement from an FMV perspective, valuation consultants are often asked to assess whether the proposed arrangement is commercially reasonable.
These reviews are very important components of a hospital’s compliance efforts. Hospitals are employing physicians on an ever increasing basis. The Stark laws require that the compensation hospitals pay to employed physicians is FMV and is part of a commercially reasonable agreement. These are separate and distinct determinations for the valuation consultant to make, because employment compensation that meets the FMV standard may not necessarily be part of a commercially reasonable agreement, and vice versa.
Determining the FMV of a physician’s services presents its own challenges, but there appears to be even more uncertainty and inconsistency in the health care valuation industry related to commercial reasonableness opinions. Part of the challenge is the limited guidance that has been provided by the Centers for Medicare and Medicaid Services (CMS) regarding the definition of “commercially reasonable” and what constitutes a commercially reasonable arrangement for physician services.
Below is a summary of the guidance that appears in the Stark regulations:
- We are interpreting “commercially reasonable” to mean that an arrangement appears to be a sensible, prudent business agreement from the perspective of the particular parties involved, even in the absence of any potential referrals.(1)
- With respect to determining what is “commercially reasonable,” any reasonable method of valuation is acceptable, and the determination should be based upon the specific business in which the parties are involved, not business in general.(2)
- In the absence of referrals, an arrangement will be considered “commercially reasonable” if the arrangement would make commercial sense when entered into by a reasonable entity of similar type and size and a reasonable physician (or family member or group practice) of similar scope and specialty, even if there were no potential DHS referrals.(3)
Without a safe harbor or universally accepted methodology available, the valuation consultant—using generally accepted approaches to valuation—must find a logical approach to determine what is commercially reasonable and then support his/her findings. A good starting point when reviewing a physician employment arrangement is to find out the purpose of the arrangement (i.e., Why is the physician being employed?) and evaluate the commercial reasonableness of the arrangement with that purpose in mind.
For example, one way to determine commercial reasonableness is to look at a physician employment arrangement as a financial investment and decide whether or not, in the absence of referrals, it is a good one. This approach works if the primary purpose of the arrangement is to produce financial returns for the hospital employer. In this scenario, benefits from the arrangement must exceed costs for a “go” versus a “no go” investment decision. The analysis consists of projecting professional collections, operating expenses, and physician expenses and then determining whether the professional services of the physician generate positive cash flows for the hospital. It is easy to argue that a rate of return in excess of the hospital’s minimum acceptable return on an investment (i.e., its hurdle rate) would make the employment arrangement commercially reasonable. The problem with this approach is that market research data indicate that the “profitable” hospital-owned physician practice is a rarity. The Medical Group Management Association (MGMA) 2018 Cost and Revenue Survey shows that the median net income/ loss for a hospital-owned family practice is a loss of $118,645 per full time (FTE) physician. For hospital-owned internal medicine practices, the median loss is $168,239 per FTE physician; for hospital-owned multi-specialty practices, the median loss is $201,703 per FTE physician. Considering this data alone, hospitals should not expect meaningful financial returns when employing physicians. Understandably, it is difficult to prove that these arrangements are commercially reasonable when analyzing them from a purely financial investment perspective.(4)
A second way to determine commercial reasonableness is to look at a physician employment arrangement and determine whether or not it constitutes a good and necessary expense for the hospital. This approach is especially appropriate if the rationale for the employment arrangement is that it helps the hospital meet the IRS’s community benefit standard for tax-exempt status or maintain compliance with other laws. An argument can be made that the employment arrangement, viewed as an expense, makes commercial sense and is a necessary cost of doing business, if the arrangement accomplishes one of these goals at a cost that is less than or consistent with other alternatives (e.g., entering into professional services arrangements with private practice physicians or recruiting new physicians to a start-up practice).
For example, the Patient Protection and Affordable Care Act (PPACA), enacted in 2010, requires that tax-exempt hospitals conduct a community health needs assessment (CHNA) every three years and adopt an implementation strategy to meet the identified community health needs.(5) These assessments often identify any community shortages of primary care physicians and specialists who accept Medicare, Medicaid, and uninsured patients and find solutions for addressing those shortages. Accordingly, fair market value compensation paid to a physician under a hospital employment arrangement may also be commercially reasonable—even if the physician’s medical practice generates a financial loss—if that arrangement helps secure or improve access to care for the Medicare, Medicaid, and uninsured populations. This may also be true for situations in which an existing non-employed community physician (1) is a roadblock to recruitment in his/her specialty, (2) won’t participate in succession planning for his/her practice, and/or (3) will not cooperate with hospital initiatives (such as quality reporting, etc.). In these cases, it may be commercially reasonable to employ the community physician (assuming that he/she will comply as a result of employment), even though the medical practice won’t generate a profit.
In any of these situations, quantifying and documenting the community benefits stemming from the physician employment arrangement and any uncompensated care the employed physician provides could be instrumental in the hospital’s efforts to maintain a tax-exempt status and could show that the arrangement is a commercially reasonable expense. Supporting documentation for the commercial reasonableness review would include analyses of the external market factors (e.g., a national or regional physician shortage, physician compensation benchmarks, recruitment offers being made to comparable physicians) that help defend the amount of compensation paid to the employed physician and show that more cost efficient alternatives were not readily available.
Another example of a physician employment arrangement that may be commercially reasonable (from the expense perspective, not the financial investment perspective) is one that does not produce a profit (from a medical practice standpoint), but does help the hospital-employer comply with the Emergency Medical Treatment and Active Labor Act (EMTALA). It stands to reason that if an employed physician’s professional services generate a loss for the medical practice, his employment arrangement could still be considered commercially reasonable, if his employment resulted in emergency coverage for a new specialty and/or reduced on-call payments to independent contractors by a substantial amount. Further evidence of commercial reasonableness would include data showing that the quality, consistency, and/or reliability of call coverage improved because of the employment arrangement.
To conclude, the commercial reasonableness of a hospital/physician employment arrangement can be determined from at least two different points of view: one in which the arrangement is viewed as a financial investment or one in which it is viewed as an expense. If the arrangement is viewed as a financial investment, it would need to produce some minimum rate of return to be deemed commercially reasonable. If the arrangement is viewed as an expense or a cost of doing business, it would need to be proven necessary and would need to be comparably priced or less costly than acceptable alternatives to be considered commercially reasonable.
These are just two examples of ways in which health care valuation consultants can assess commercial reasonableness. As previously noted, CMS has indicated that any reasonable method of valuation is acceptable, thus implying that there are many other valid approaches, including those that seek to quantify the value of the community benefit (such as increased access to quality care) that can come from hospital/physician employment arrangements. Regardless of the approach used, a commercial reasonableness analysis requires an understanding of the purpose of the arrangement being reviewed; acknowledgement of the relevant facts and circumstances of the situation; and an appreciation of the unique requirements and needs of the hospital, the physician, and the community involved.
- Federal Register / Vol. 63, No. 6 / Friday, January 9, 1998 / Proposed Rules
- Federal Register / Vol. 66, No. 3 / Thursday, January 4, 2001 / Rules and Regulations
- Federal Register / Vol. 69, No. 59 / Friday, March 26, 2004 / Rules and Regulations
- Medical Group Management Association, 2018 Cost and Revenue Survey
- U.S. House of Representatives, 111th Congress, 2d Session PRINT 111–1, Compilation of Patient Protection and Affordable Care Act, U.S. House of Representatives, May 2010
This article was originally published in the July 2011 (Volume 13 Number 7) issue of Compliance Today. It has been updated to reflect 2018 data.

We ranked the 30 largest healthcare services and information technology deals of 2018, according to our database, by valuation multiple. The lowest reported price to EBITDA multiples (10x or lower, sorted alphabetically) are listed below.

We ranked the 30 largest healthcare services and information technology deals of 2018, according to our database, by valuation multiple.

We ranked the 30 largest healthcare services and information technology deals of 2018, according to our database, by valuation multiple. The highest reported price to EBITDA multiples (15x or higher, sorted alphabetically) were as follows:

Healthcare services organizations rely on a variety of intangible assets to create business value, including patient and customer relationships, medical records, trade names, assembled workforce, licenses and certifications, non-compete clauses, proprietary technology, software, and others.

For those of you who’ve been involved in a transaction where the only asset transferred is a certificate of need, you’ve probably found that market data is scarce for CON-only deals.

CON Laws, Scope of Practice Restrictions, and Provider Non-Compete Clauses Targeted in New Trump Adm
On Monday, December 3, 2018, the Department of Health and Human Services (HHS) – in collaboration with the Departments of the Treasury and Labor, the Federal Trade Commission, and several offices within the White House – released a report detailing recommendations for improving choice and competition in the healthcare industry.

One of the questions we get asked a lot is how valuations have changed over time.

One of the many benefits of tracking healthcare transactions closely and maintaining a very large database of deals where we can get reliable price to EBITDA and revenue multiples is that it provides insight into profit margins for segments where other financial benchmarking information is sparse.

The most important component of a valuation of an accountable care organization (or other multi-provider network that relies on risk-based shared savings models) is the revenue forecast, which involves “probability-adjusting” future shared savings payments in some manner.
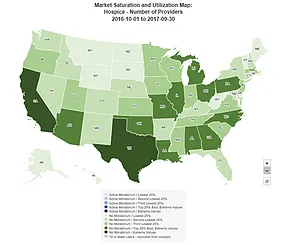
CMS' offers a helpful online tool that shows provider market saturation levels at the national-, state-, and county-levels for the following health services:

